Captain Morris J. Gilbert was the Steward of The Willard Asylum for the Insane from 1873 until his death in 1901. According to Dr. Robert E. Doran, Jr., author of History Of The Willard Asylum For The Insane And The Willard State Hospital, “he was totally responsible for all purchasing as well as overseeing the farm and maintenance work.” “Report after report by different Superintendents and various Boards of Trustees or Managers speak very highly of his ability and integrity.” Willard and all New York State Asylums employed a steward. These institutions would not have been able to function without the steward running the day to day operations of the farm, garden, various workshops and overall maintenance of the buildings and property. The asylums were like villages that tried to be as self-sustaining as possible. Employees lived on the asylum property and were supplied with room and board in addition to very low wages. I have featured an excerpt from Dr. Doran’s wonderful, insightful, detailed work that sheds a great deal of light on the inner workings of how Willard operated. I have also included a few excerpts and photographs from various sources about Captain Gilbert and his extensive job duties as the steward.

Captain Morris J. Gilbert – Wayne E. Morrison, Sr. 1978
“I wish to say that I am particularly pleased to report one small matter, but one worthy of some attention, and that is, that during the past year we were able to get the Lehigh Valley railroad to change the name of the station formerly known as ‘Willard’ by naming it ‘Gilbert,’ after Captain Gilbert, who has been for so many years connected with the hospital. The name of the station at the hospital proper is also changed from ‘Asylum’ to ‘Willard.’ This change obviates a very annoying complication that has previously come from the wrong ideas that people got who wanted to come to the hospital from a distance, because of the peculiar name of these stations. Generally outsiders expected that the station known as ‘Willard’ was right at the hospital, and many of them would go there, not knowing it was over a mile away from the hospital, while the name ‘Asylum’ clinging to the locality years after the name of the institution itself had been changed to hospital, was something that we had long wished to have changed. The railroad has finally made the substitution in the name as described, and now those coming to Willard arrive at a little station that the railroad people built upon the grounds, only a short distance from the hospital, to which a cement walk leads directly.” –William Austin Macy, Medical Superintendent, 1900. (1)
According to The New York Times, published: October 24, 1901: “MORRIS J. GILBERT, for the past thirty-five years Superintendent of the State Hospital for the Insane at Willard, Seneca Lake, N.Y., died on Tuesday at Willard, after a long illness. Mr. Gilbert was sixty-nine years old, and is survived by his widow, two sons, and one daughter. One of the sons is the Rev. William Morris Gilbert, rector of St. Paul’s Church, Yonkers.” (2) NOTE: Mr. Gilbert was the Steward not the Superintendent. He held that position for 28 years.

Residence Of Cap’t Morris J. Gilbert, Asylum Steward – Wayne E. Morrison, Sr. 1978
“Farms and Industries: For a great many years, the Institution tried to be as near self-supporting as possible. The first report of the Trustees dated February 18, 1868, states that the sum of $1,000 had been received from the State Controller. Of this, $916.66 had been expended in preparing the ground, procuring the seed and sewing sixty acres of wheat. They hoped for a good crop. By the time the Asylum opened, there were 475 acres under cultivation. A Steward had been appointed and a Matron. The former was an ancient title for one who managed a feudal estate. His duties at Willard were many and important. For about the first fifty years, he did all the purchasing, supervised the farm and garden operations, the upkeep of the buildings and grounds, the distribution of supplies, and the overseeing of the various industries. The Matron was in charge of housekeeping, the sewing room, and, in the early days, the care of the sick. As early as 1870, 3,429 pieces of clothing were made, and, up until 1912 when the position was abolished, she was in charge of the kitchens and dining rooms.
The farm and gardens were never able to completely supply the needs of the Institution but they made a very large contribution. The garden extended from east of the Maples to the Hermitage with berry bushes and strawberries where the golf course was later laid out. The land was not particularly good but was gradually improved. When Captain Morris Gilbert was appointed Steward in 1873, he asked for more land as there was not enough for hay and pastures. Four years later, 258 acres were acquired at $105 an acre. Beside the farm and gardens, there were other uses for the land. The bricks for the early buildings were made on the grounds at a yard located at the site of the reservoir. Lime was made and stone quarried. It so happened that there was an outcropping of Tully limestone in Simpson’s Creek ravine. The stone was used for lime, foundations and later as crushed stone for the roads. At first, only the main road was of this material. Secondary roads were of shale which outcropped above and below the limestone. It was many years before all roads were made hard. At one time, a roadroller was borrowed from the Binghamton State Hospital, but this didn’t work out as both Institutions needed it at the same time. A steam roadroller was acquired which served several uses. It powered the rock crusher which stood in the ravine south of the reservoir. There was a little brick house near it where dynamite was kept for blasting. The roadroller also powered the threshing machine and a portable sawmill. For years, fallen timber and diseased trees were sawed, the lumber being used for various repairs and construction. Enough black walnut stock was built up to swap it for pine and maple boards. The slabs from the mill were made into bushel crates for potatoes and other vegetables. The sawdust was used in the icehouses and sometimes in the pigpens.

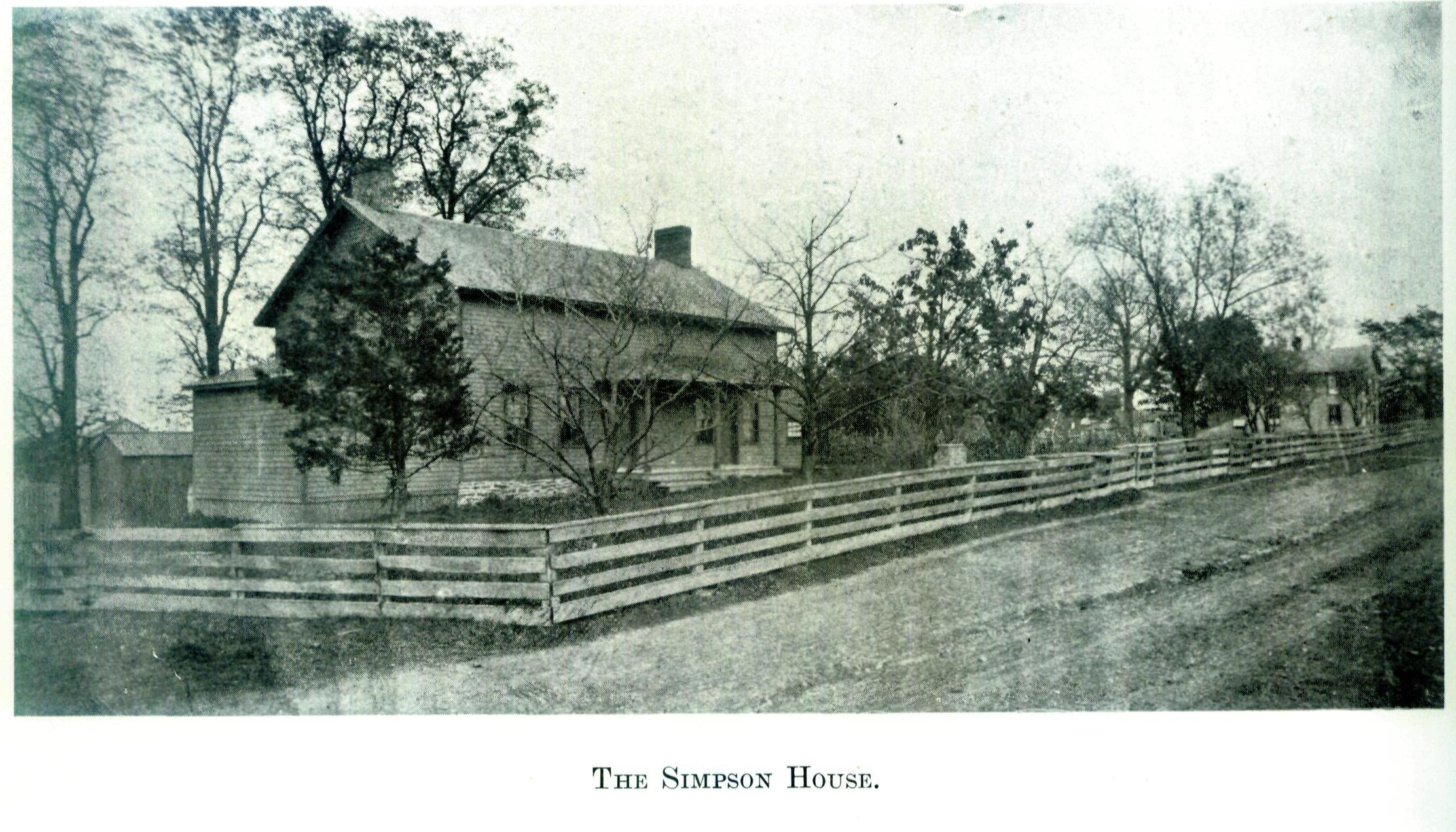
The Simpson House – Wayne E. Morrison, Sr. 1978
Ice was supplied from the upper reservoir and pond. This was drawn in wagons and sleds to the icehouses. There was one just west of the present Elliot Hall which was also used for cold storage. Another later became the tinsmith shop, below and south of Hadley Hall. There were icehouses in the vicinity of the barns, and we hear of new ones being built of hollow concrete blocks. In 1917, there were four of these icehouses. Ice was harvested long after the plant for artificial ice was in use. There were a couple of poor years, but in the winter of 1919 the ice was 30-34 inches thick and 1,200 tons was cut. Needless to say, this ice could only be used for cooling in refrigerators or cold rooms and not for consumption.

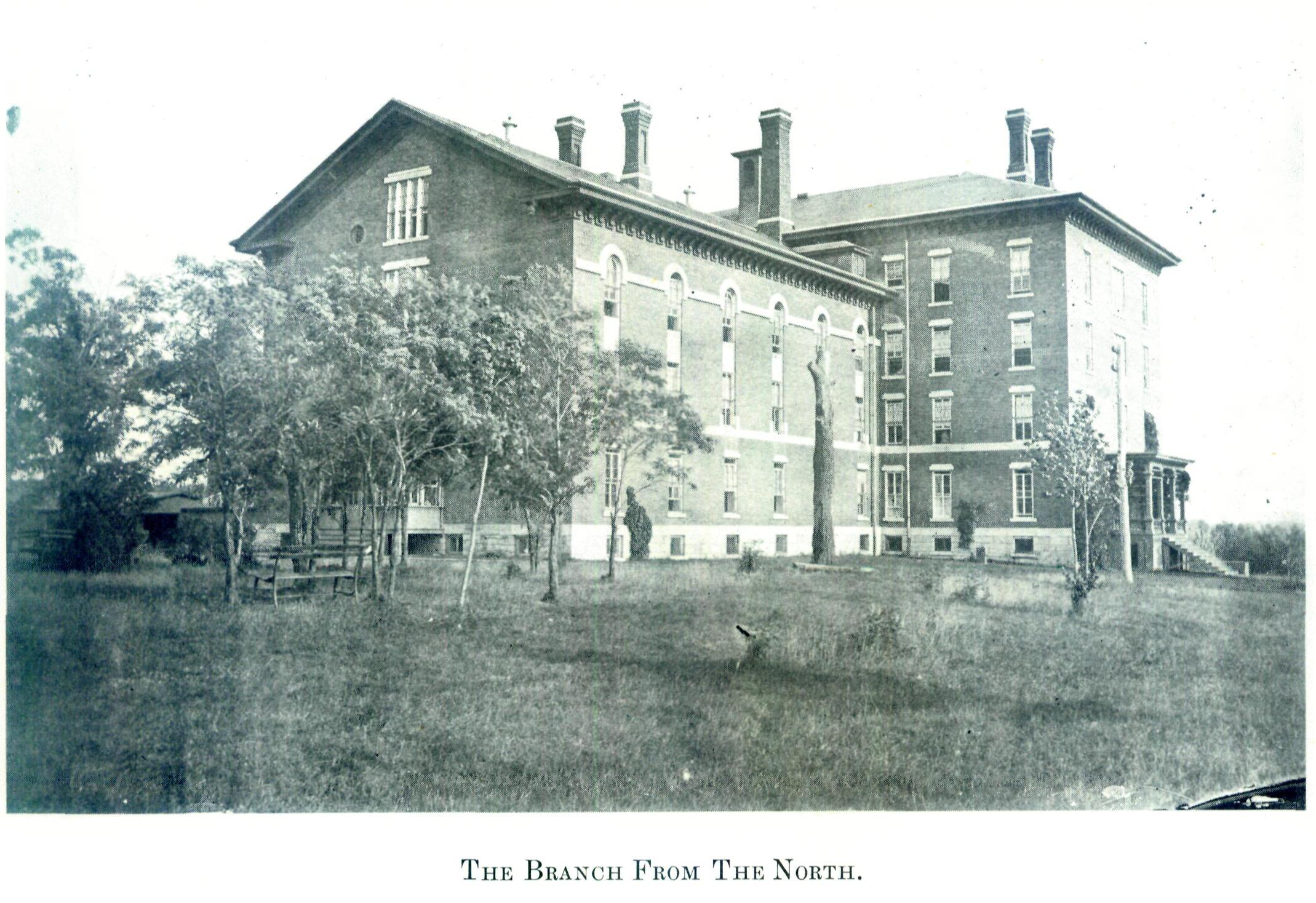
The Branch, Barns, &c., From The Simpson House – Wayne E. Morrison, Sr. 1978
The piggery was an important resource. As early as 1870, 4,400 pounds of pork was produced. Ten years later, 50,750 pounds at 6¢ a pound was worth $3,045. This was not without its drawback. The piggery and slaughterhouse was located near where the County Road crosses the creek and not far from Sunnycroft. It was also near the Simpson’s house to the south. Between the pigs, the slaughterhouse, the tallow rendering plant and the fact that sewage was being dumped into the creek, the Simpson’s were unhappy. In 1884, the farm of 135 acres along the south side of the creek with three dwelling houses was bought for $10,298.40. Appropriately enough, this sum had been accumulated by the sale of hides, bones, tallow and rags. In 1893, request was made to move the piggery and slaughterhouse; the lake farm was suggested as a site, but this was impractical because no railroad track was available to take the garbage there. Four years later, the pigs were moved east of the railroad cut, far enough away not to be a nuisance. While swine seemed to be freer of disease than cattle, there was a serious outbreak of swine flu or hog cholera in 1915 when 200 pigs were lost. Pork continued to be an important product. In 1960, 91,221 pounds was reported as worth $27,366.30. The next year the farm came to an end.
The dairy herd was the backbone of the farm. Starting with 1,800 quarts of milk 4 in 1870, we find over ten times that much ten years later. In 1873, the entire here had to be slaughtered because of tuberculosis and in 1883 50% were killed. It was during this decade that it was proved that bovine tuberculosis could infect human beings. The cows that formed the herd had been bought locally from various farms. It was now decided to breed their own stock from hopefully healthy animals. This seemed to work well for twenty years or more, but in 1908 sixty cows reacted to the tuberculin test. The cows were Holstein but not thoroughbreds. In 1915, the thoroughbred herd was started. All was not well as five years later out of 134 cows, 124 were positive, and out of 91 heifers, 30 were positive. The managers felt that part of this was due to improper supervision which was probably true during the war years. They asked an appropriation of $20,000 to build a new herd. By 1925, milking machines were being introduced. The pasteurizing plant had been installed previously. In 1937, the New York State Department of Agriculture and Markets gave the following figures for milk produced: The average production in the years from 1923 to 1935 was 8,334 pounds per cow. In the year 1936, it jumped up to 10,733. By 1940, the value of milk produced was $44,579. It was a good thing that it was high and that the farm as a whole was extending itself to the utmost. The next five years were war years with rationing and food shortages. Thanks very largely to the farm, the patients were well cared for. In 1945, the milk production was 727,571 quarts and the next year the average per cow was 12,000 pounds per year. Dr. Keil was proud of the herd and states that the State average was 6,000 pounds per year. Four years later he reports that there were 275 cows, that 15 of them gave better than 15,000 pounds a year and that one gave 18,950 pounds a year.
There was much sadness when the Department of Mental Hygiene, on order it is understood from the Governor, announced late in 1960 the closing down of the farm. The Board of Visitors unanimously opposed the idea and so did almost everyone else. For over 90 years the herd fully supplied the Institutional needs for milk. This was not true of butter and cheese. The audit of 1886 shows that butter was bought from dozens of people in small amounts. To a lesser extent, this was true of cheese.
Much of the work at the farm was to support the dairy herd. There was good pasture in season. The cows grazed in fields each side of the road running to Grandview above the County Road. Much corn was raised for ensilage, and we read from time to time of the need for more silos. Mangel-wurtzel was raised by the thousands of bushels. Alfalfa was introduced early in the century and was considered a wonder crop. The wheat raised was sent by rail to a mill and the flour returned was used in the bakery and bran fed to the stock.
Considerable beef was produced. For instance, in 1890 there was 4,714 pounds of dressed beef, and in 1934 there was 28,510 pounds. Hay and oats were raised for the horses of which at the turn of the century there were 27 plus 9 colts and one mule. There were also 24 sheep, 11 lambs; 60 turkeys, 7 geese, 30 ducks, and 260 foul completed the bird census. Sometimes there were peafowl, and for a long time there was a span of oxen. Up until 1926, there were driving horses which were called “administration horses.” They numbered a dozen or more, but in that year the automobiles took over. Farm horses hung on much longer. A Holt caterpillar tractor was bought in 1915. Mr. Warren, the Steward, was very pleased with it, stating that it could do the work of from eight to ten teams. Two years later, he again tells of it and states that, even with gasoline at the very high price of 25¢ a gallon, it was an economy.
On going over the annual reports of the Steward, one learns of the good weather and the bad, of the droughts, floods, hailstorms and tempests that occur. The latter two were particularly hard on the orchards of which there were about 120 acres. From the very start, apples had been a good crop and supplied the cider and all the vinegar for the hospital. Grapes became a big crop, large enough to give all the patients grapes everyday during the season. Some years, the grapes were exchanged on the market for oranges so that the patients could have them at Christmas time. Concords, Niagaras, Delawares and Catawbas were grown, mostly east of Edgemere or around Vinelands. The orchards also were in this general vicinity, but there were fruit trees on the lake farm back of Buttonwood.
The poultry was concentrated near Vinelands to the south, but there were some at Hillside. In 1937, there were 2,324 pounds of dressed chicken and 1,503 dozen eggs. In 194?, the egg output was reported at an all time high of 8,136 dozen.
The garden produced all the vegetables with the exception of onions and potatoes, the soil not being suitable for the former and not too good for the latter. Even so, there were years when there was a respectable potato crop. For instance, 3,850 bushels were produced in 1933.
In the early years of the century, there was a canning plant in the old warehouse located on the steamboat dock. The reports often mentioning canning and evaporating as important activities. In the 1917 report, it is broken down into categories: Canned apples 1,043 gallons, plums 914 gallons, pears 2,329 gallons, peaches 1,962 gallons and tomatoes 1,584 gallons. The evaporating apparatus was in the old pump house near the State dock. That year, 225 pounds of raspberries were dried and the dried weight of sweet corn was 1,935 pounds. This was put up in empty sugar and cracker barrels.
The garden grew everything from asparagus to vegetable oysters of which there were over six tons in 1931. The demands of the Institution at that time were for over 3,000 people.
The farm and garden always made a profit – sometimes more, sometimes less – depending on the weather and the amount of supervisory help available. As most of the work was done by the patients, good supervision was necessary.
Willard not only raised food, but also manufactured articles for the care and maintenance of the patients. There were a number of shops where a large part of the work was done by the patients, to their great benefit. A look at the figures from year to year is most instructive. The shoe shop at first spent most of its energy repairing shoes and making and repairing harness. This shop was also responsible for making and repairing mattresses. In 1895, the bulk of the articles made were mattresses, hair pill and harness, with boots, shoes and slippers repaired in quantity. By 1912, after shoemaking machinery had been acquired, 2,579 pairs of boots and shoes were made. In 1932, the shoe and mattress shop made 4,682 articles and repaired 3,286. Twenty years later, the shop wasn’t making as many shoes but it was still very busy. Seventy years ago, there were canaries in cages on many of the wards. For some reason, the shoe shop had many cages of them. Perhaps, they took the place of piped-in music. The shop was located on the second floor of the storehouse on the east side. The mattress shop was adjoining.

Interior Of The Shoe-Shop – Wayne E. Morrison, Sr. 1978
The sewing room was probably the first industry. It turned out articles by the thousands, as did the tailor shop which was adjoining. In 1885, the sewing room turned out over 20,000 articles and the tailor shop 5,841. Besides this, there were almost 9,000 sheets, towels and pillow covers made. In 1893, over 4,000 wrappers or aprons were made and 4,000 dresses, and almost as many skirts. For some reason, there were over 3,000 collars made, which seems like a strange item. The tailor shop in the same year made about 1,500 coats and over 2,000 pants, and 1,500 vests which must have been in the style at the time. In 1926, they were still going strong, making nightgowns by the thousands, 2,500 chemises; in other words, they were making practically all the clothes for the patients. It was a time when male employees, nurses and attendants, wore blue uniforms made from Metropolitan Police blue cloth. These were made in the tailor shop and sold at cost. In 1953, the sewing room made over 50,000 articles and repaired 10,000 the tailor shop made about 11,500.
Another busy industry was the broom shop which made brooms by the thousands as well as brushes, baskets, crates, doormats and floor polishers. Chairs were caned and furniture repaired. Floor polishers were an important item as the floors all over the hospital were kept polished to the “nth” degree. An attendant would spread wax on the floor by scraping a block of paraffin with a metal comb. The patients would shove the polishers back and forth by the hour. At the Hermitage, the day room was so large that a polisher about four feet square was pulled back and forth by ropes. It was weighted down by a patient sitting in a chair on top of it.

The Basket, Mat & Brush Shop – Wayne E. Morrison, Sr. 1978
The tin shop was another busy place; probably not as many patients were employed here as in other shops. The number of different articles made here is astonishing. Some years, over 75 different categories are listed – everything from bird cages to a two foot ventilator with hood for the Nautilus boathouse, boxes, basins, boilers, cups, chamber pots, cans, dippers, measures, pails, pots, pans, strainers, trays, etc. They also made yards and yards of eaves troughs and conductor pipe.
Taking a typical year, we might look at the value of articles made by patients. In 1955, the value was $50,427.28; in the same year the value of farm and garden produce used for food was $173,303.70.
Until very recently, the bakeries at Willard made all the bread for the Institution. During the late 1940’s, a new type of bread was developed at Willard in conjunction with nutritional experts from Cornell. This came to be called Willard Bread. It was a rich protein type of bread to which soy bean flour was added and also vitamins.
Of the Stewards who served Willard, three stand out for their length of service and ability. Captain Morris Gilbert was in office from 1873 until his death in 1901. During that time he was totally responsible for all purchasing as well as overseeing the farm and maintenance work. Report after report by different Superintendents and various Boards of Trustees or Managers speak very highly of his ability and integrity. When he died, Dr. Macy had to take a man from Civil Service who had had no experience with a farm. After a short term, he resigned, frankly stating that he didn’t have what it took. Mr. Frank Warne was appointed in 1902, serving with great ability until his retirement in 1934. His annual reports are of considerable interest in recording the various trials and triumphs of the farm. Mr. Samuel Peltz was appointed in January, 1936, and served until his untimely end September, 1954; he was highly regarded and well liked. It was fitting that the new storehouse building was named in his memory. These three men served a total of 75 years.” (3)
1900 Report of Steward (4) Transcribed by L.S. Stuhler
SOURCES:
(1) Thirty Second Annual Report of the Board of Managers of the Willard State Hospital to the State Commission in Lunacy for the Year 1900, Chapter 20 Report of the Board of Managers of the Willard State Hospital.
(2) The New York Times, Published: October 24, 1901. Copyright@TheNewYorkTimes
(3) History Of The Willard Asylum For The Insane And The Willard State Hospital by Robert E. Doran, M.D., 1978, Pages 36 – 42. About Dr. Robert E. Doran, Jr. in his own words: “INTRODUCTION: The author of this little history of Willard lived there as a little boy when my father was First Assistant physician. Later, I made frequent visits to the place and became consulting surgeon there in 1934. My contacts with the Institution cover about two-thirds of its existence. I wish to express my thanks to Dr. Anthony Mustille who has been supportive of this history and made available the services of Mrs. Maurita Lind who has been most helpful in furnishing me with reports, articles, laws and other material. Mr. J.F. McCauley, Deputy Director for Administration, furnished me with a resume of the regulations pertaining to patient employment. Miss Helen B. Vincent, Principal of the School of Nursing, has given me information about it and its impending disestablishment.”
(4) Reprinted from Thirty Second Annual Report of the Board of Managers of the Willard State Hospital to the State Commission in Lunacy for the Year 1900, Chapter 20 Report of the Board of Managers of the Willard State Hospital, Pages 297-306, 308, 309, 310, 311, 312.
(5) Photographs – Morrison, Wayne E., Pictorial Album of The Willard Asylum 1869 – 1886, 1978.