Rochester State Hospital, formerly Monroe County Insane Asylum
Rochester, Monroe County, New York
1600 South Avenue
The history of the Rochester State Hospital is a little confusing because the lines blur between the Alms House and the Insane Asylum which would later be known as the Rochester State Hospital. Four structures stood on the same tract of land, facing South Avenue, between Elmwood and Highland Avenues, in the Town of Brighton. None of these structures remain. The original Monroe County Poor House or Alms House was built in 1826. The Work House was built in 1853 at the cost of $22,707.60 and contained ninety-two cells for men, women, and occasionally children. In 1865 and again in 1868, fires broke out and the buildings were replaced. In 1869, new brick buildings were constructed. At some point the Work House was renamed, the Penitentiary. Before county “Insane Asylums” the “insane” were kept in jails and county poor houses, separated from the other inmates and usually in chains or handcuffs. The first buildings of the Monroe County Insane Asylum were opened in the spring of 1857. It is at this point that the lines become blurred because the official year of the opening of the asylum is 1863.
According to W.H. McIntosh: In 1856, “there were thirty-seven insane confined in thirteen cells [in the alms house]. These cells were low, unventilated, and unwholesome, and in dimensions but four and a half by seven feet. In this small space were crowded as many as four persons, some of whom, wild and raving, were chained and handcuffed. There was no out-yard, and no guards to stoves to prevent self-inflicted injury. It was resolved to erect a permanent and convenient building especially for the insane. It was constructed at a cost of somewhat over three thousand dollars, during 1856 and 1857.” (1) The Monroe County Insane Asylum opened in the spring of 1857 to accommodate forty-eight people and was under the supervision of Colonel J.P. Wiggins and wife. An additional wing to house the superintendent and employees was completed in October 1859 at a cost of $26,791.57. Because of the lack of room, several patients still remained in the Poor House. In 1870, an additional wing was constructed to accommodate twenty-five more patients. In 1871, the number of inmates rose to one hundred. In 1872 an entirely new, main building was constructed with forty-one rooms at the cost of $18,000, and with various improvements close to $50,000. Dr. M.L. Lord was the warden and physician beginning in 1868.
According to the 1872 Proceedings of the Board of Supervisors of the County of Monroe: “Your Committee in tracing back the history of Monroe County Insane Asylum to 1863, when, by an act of the Legislature, it was made a separate institution from the County Alms House, find that the whole number of inmates supported at that institution during the year was sixty-three. The number of inmates now in that institution have increased to 137, and has more than doubled during the last nine years…” (3, page 18).
The Alms House – In 1860, a building, “was set apart for the infirm old men.” (1) George E. McGonigal was the Superintendent, and Dr. Azel Backus was the physician. On February 28, 1872, a building committee was appointed for a new almshouse to be built at the cost of $59,600. “The almshouse was located midway between the insane asylum and the penitentiary, and fifty feet south. The architect employed was J.R. Thomas. The entire cost of the work was $72,948.44.” (1) In late 1872, the new Monroe County Alms House was completed and opened. It was built in front of the old and at some point thereafter, the original poor house was torn down.
The Insane Asylum – The State of New York purchased the land and the buildings of the Monroe County Insane Asylum for $50,000 bringing it into the State Care system. On July 1, 1891, it was renamed, Rochester State Hospital. Dr. Eugene H. Howard was the first Superintendent and served in that position for several years. (2) The Rochester State Hospital was torn down in the 1960s to make way for The Al Sigl Center. Rochester State Hospital faced South Avenue, the address was 1600 South Avenue. The Al Sigl Center faces Elmwood Avenue, the address is 1000 Elmwood Avenue.
So it appears that in 1857 a separate building was constructed for the sole purpose of becoming the Monroe County Insane Asylum. In 1863, by an act of the New York State Legislature, the asylum was officially separated from the alms house. In late 1872, the NEW Alms House was opened. In that same year, an entirely NEW main building was constructed for the Insane Asylum complete with a Mansard Roof. If you look at the sketch of these three buildings (W.H. McIntosh’s book of 1877), you can see that all three are separate but they stand side by side, three in a row: Far left, Penitentiary; Center, Alms House; Far right, Insane Asylum.

Work House, County Infirmary, Insane Asylum 1877
There is an interesting map that was drawn in 1984 during an excavation of Highland Park that shows the footprints of the original wood frame and brick buildings. At this time, the remains of approximately 900 people were discovered. (4) In April 2013, while researching the history of the poor house and the asylum, I came across the “Chaplain’s Report” from 1872 which stated that the unmarked cemetery, “familiarly known as the ‘bone yard,” was “an enclosed lot of the public farm in the rear of the penitentiary.” (3) This cemetery was located behind the old Penitentiary and was used to bury the inmates of the Penitentiary, Alms House, and Insane Asylum from 1826 until January 8, 1873 when the County Board of Supervisors directed the Superintendents of the Penitentiary and of the County Poor, “to discontinue the burial of paupers or criminals in the old burying ground attached to the penitentiary, and to have the remains of all such interred in Mount Hope cemetery.” (3) The county board of supervisors of 1872 were well aware that this cemetery existed but apparently, it was never recorded. Perhaps the document concerning this cemetery hasn’t been discovered yet. The Remember Garden in Highland Park marks the location of this long forgotten cemetery.
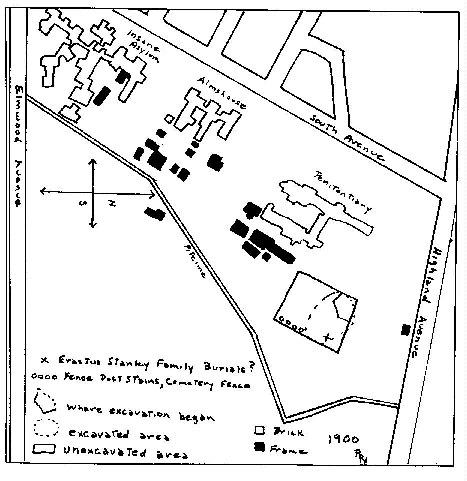
Map of Penitentiary, Poorhouse, Asylum
305 bodies were interred at Mount Hope Cemetery in 1985. The remaining bodies (approximately 600) (4) were left in the ground at Highland Park. The picture below shows a man preparing the ground for the monument that was or will be placed in memory of these original inmates. There is NO monument in Mount Hope Cemetery for the inmates of The Monroe County Insane Asylum / Rochester State Hospital, most of whom were buried in anonymous, unmarked graves in Section Y. If bill S2514-2013, which was introduced to the New York State Legislature by Senator Joseph Robach, becomes a law, then these people will no longer be anonymous.

Mount Hope Cemetery 11.2011
“Work is now underway to install a monument in memory of the 305 Rochester poor house remains now interred in Mount Hope Cemetery. From the picture you can determine that the monument is in Section Y at the far west end. Note the Civil War plot, the Fireman’s monument and the Steam Gauge and Lantern Co. monument in the background. In July, 1984 when terracing land for a Highland Park addition, a bulldozer unearthed some human remains near the SE corner of Highland and South Ave. Investigation proved these burials were very old. It is believed they are from the Rochester poor house. The burials were not marked and the people were interred in the most simple wooden coffins. These remains underwent an examination prior to their reburial in Mount Hope Cemetery.” 11/2011
I have transcribed the earliest records: Names: Monroe County Poorhouse, Asylum, Penitentiary, Other Charities 1838 to 1860. If you believe that your ancestor was an inmate who lived and died at The Monroe County Insane Asylum / Rochester State Hospital you can search for them at the Rochester – Mt. Hope Cemetery Records online. Here is a brief description of what you will see if you decide to search the records for yourself: Under the heading “Residence,” a street name will be given with no specific address; or it will list the place where the person died such as: Insane Asylum, Asylum, County House, Jail, etc. (Be aware that there was an Asylum Street in the City of Rochester that as far as I know, had no connection with the Monroe County Insane Asylum). About 1891, you will start to see the words “Rochester State Hospital” under “Residence.” At some point in the 1900s, instead of listing the place of death as Rochester State Hospital the address has been given instead as “1600 South Avenue.” In some instances, the family of the deceased claimed the body and buried them in the family plot. In the case of pauper and indigent insane, the hospital buried them in unmarked, anonymous graves at Mount Hope Cemetery. Some unclaimed bodies were donated by state hospitals to state medical colleges for the advancement of medical science in which case no grave will be found.
SOURCES:
1 – McIntosh, W.H., History of Monroe County, New York; With Illustrations Descriptive Of Its Scenery, Palatial Residences, Public Buildings, Fine Blocks, and Important Manufactories, From Original Sketches By Artists Of The Highest Ability. Philadelphia: Everts, Ensign & Everts, 1877, Pages 45-47, Transcribed by L.S. Stuhler.
2 – Hurd, Henry Mills; Drewry, William Francis; Dewey, Richard; Pilgrim, Charles Winfield; Blumer, George Adler, The Institutional Care of the Insane in the United States and Canada, The John Hopkins Press, Baltimore, Maryland, 1916, Pages 199-200, Transcribed by L.S. Stuhler.
3. – Proceedings of the Board of Supervisors of the County of Monroe, for 1872, Rochester, N.Y., Steam Press of Curtis, Morey & Co., Union And Advertiser Office, 1872, Pages 18, 211, 212.
4. – Steckel, Richard H. and Rose, Jerome C., The Backbone of History: Health and Nurtrition in the Western Hemisphere, Cambridge University Press, 2002, Page 162.
Friends of Mt. Hope Cemetery – The Friends of Mount Hope Cemetery are a wonderful group of knowledgeable volunteers who will help you locate your loved one and provide you with all the information you need to locate the grave.
Facebook – Friends of Mt. Hope
USGenWeb Monroe County, NY – Mt. Hope Cemetery Tombstone Transcriptions
Records of the Rochester State Hospital
Photographs of Memorial to Residents of Almshouse, Insane Asylum & Penitentiary by L.S. Stuhler
History of Mount Hope Cemetery – McIntosh 1877
Rochester History – Life and Death in Nineteenth Century Rochester by Ruth Rosenberg-Naparsteck, pages 12 – 22.
1872 “Bone Yard” – The Remember Garden – Rochester, NY by L.S. Stuhler
1873 Monroe County Poor House
The Willard and Rochester State Hospital Connection by L.S. Stuhler
CLICK HERE TO VIEW THE VIDEO They’re Buried Where? by Seth Voorhees
The Inmates Of Willard 1870 to 1900 A Genealogy Resource by L.S. Stuhler




